Researchers at Rush University Medical Center have found that injecting tumors with influenza vaccines, including some FDA-approved seasonal flu shots, turns "cold" tumors to "hot," a discovery that could lead to an immunotherapy to treat cancer. The study results were published Dec. 30 in the Proceedings of the National Academy of Sciences.
Changing the microenvironment of tumors to increase the immune system’s response to them has been the goal of countless research and clinical studies including the most recent use of checkpoint inhibitory antibodies. The majority of patients have tumors that are “cold” — that is, the tumors don’t contain many immune cells, or they have cells that suppress the ability of the immune system to fight them.
Increasing immune cells within a tumor can change it from “cold” to “hot” — more recognizable to the immune system. Hot tumors show higher rates of response to treatment, and patients with such tumors have improved survival rates.
Inactivated flu vaccines can make tumors hot
Currently, some immunotherapies utilize live pathogens (disease-causing organisms) as cancer treatments, but these treatments only have shown lasting effects in a limited number of patients and cancer types. “We wanted to understand how our strong immune responses against pathogens like influenza and their components could improve our much weaker immune response against some tumors,” said Andrew Zloza, MD, PhD, assistant professor in Rush Medical College’s Department of Internal Medicine and senior author of the study.
Drawing on a National Cancer Institute database, researchers found that people who had lung cancer and hospitalization for a lung infection from influenza at the same time lived longer than those who had lung cancer with no influenza. They found a similar outcome in mice with tumors and influenza infection in the lung.
“However, there are many factors we do not understand about live infections, and this effect does not repeat in tumors where influenza infections do not naturally occur, like skin,” Zloza said.
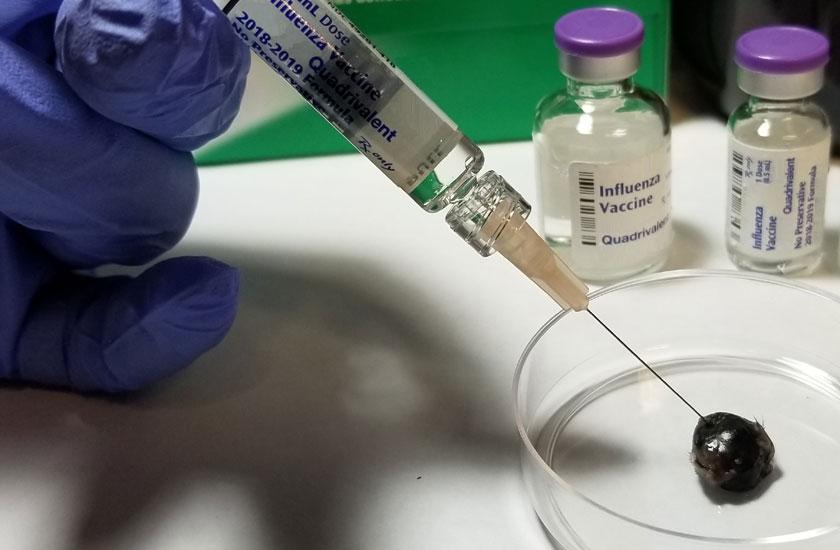
To find an alternative to the limitations of live infection, researchers inactivated the influenza virus, essentially creating a flu vaccine.
They found that direct injection of this vaccine into the skin melanoma of the mice resulted in the tumors either growing slower or shrinking. The injection made the tumor hot by increasing the proportion of a type of immune-stimulating cells (called dendritic cells) in the tumor, leading to an increase in a type of cells known as CD8+ T cells, which recognize and kill tumor cells.
Importantly, injecting a skin melanoma tumor on one side of the body not only resulted in the reduced growth of that tumor, but also in reduced growth of a second skin tumor on the other side of the same mouse that was not injected.
The study authors note that they observed similar systemic outcomes in a mouse model of metastatic triple-negative breast cancer, in which both primary tumor growth and the natural spread of the breast tumor to the lungs were reduced after injection only into the primary tumor. “Based on this result, we hope that in patients, injecting one tumor with an influenza vaccine with lead to immune responses in their other tumors as well,” Zloza said.
FDA-approved flu shots also reduced tumor growth
“Our successes with a flu vaccine that we created made us wonder if seasonal flu vaccines that are already FDA-approved could be repurposed as treatments for cancer,” Zloza said. “Since these have been used in millions of people and have already been shown to be safe, we thought using flu shots to treat cancer could be brought to patients quickly.”
The researchers found that injection of such flu shots also resulted in reduction of tumor growth.
To determine if similar results could be obtained with tumors from patients, the researchers developed a mouse model, which they call AIR-PDX. To create this model, they implant a piece of tumor and immune cells from a patient with cancer into a mouse that does not have a functioning immune system of its own – which prevents the mouse from rejecting the implanted cells.
“Such transplant allows us to utilize patient-grade drugs in a living system. This is as close as we can get to testing something ahead of a clinical trial,” Zloza said.
The researchers used a patient’s lung tumor and a melanoma metastasis in AIR-PDX models. They found that putting the flu shot in these patient-derived tumors causes them to shrink, while untreated tumors continued to grow.
Influenza vaccines can be combined with immunotherapy
Since new treatments are often compared to or combined with current frontline therapies for cancer, the researchers used immune checkpoint inhibitors in their studies. Immune checkpoint inhibition “releases the brakes” on immune cells so that they can fight the tumor.
The researchers found that flu vaccines can reduce tumor growth when used alone, whether or not the tumor is responsive to checkpoint inhibitor therapy. When they combined the flu vaccine with a checkpoint inhibitor together, an even a greater reduction in tumor growth occurred.
“These results propose that eventually both patients who respond and who do not respond to other immunotherapies might benefit from the injection of influenza vaccines into the tumor, and it may increase the small proportion of patients that are now long-term responders to immunotherapies,” Zloza said.
Not all effective flu vaccines work on cancer
Five different influenza shots for the 2017-2018 flu season were used in this research. Four were effective in achieving the same results in fighting tumors.
One flu shot with a synthetic adjuvant (an immune modifier) had no antitumor effect, and maintained other cells (called regulatory B cells or Bregs) that suppress an immune response. When the adjuvant was removed from the vaccine, it became effective. Similarly, when the B cells were removed, the vaccine also then became effective.
That all five vaccines provided protection from flu infection, but one was ineffective in reducing tumor growth “demonstrates a disconnect between the principals of immune responses needed to fight pathogens versus tumors,” Zloza said. “It also highlights the need for additional consideration regarding what adjuvants are included in immunotherapies and which vaccines could be used to treat cancer.”
Flu vaccine’s FDA approval may speed clinical trials
“Since humans and mice are about 95% genetically identical, the hope is that this approach will work in patients. The next step planned is to conduct clinical trials to test various factors,” Zloza said.
Clinical trials on average require four phases and can take between eight to 10 years to complete, but because the seasonal influenza vaccine is FDA-approved, the clinical trials for this study might be significantly shorter. “Although we are currently studying the use of other vaccines as well, the seasonal flu shot is safe and recommended for most people over 6 months of age, including most patients with cancer,” Zloza said. “This is why we chose to start with it.
“The flu shot is inexpensive and it has a quick translatability since it is an FDA-approved drug that we are repurposing,” Zloza continued.
Jochen Reiser, MD, PhD, a professor in Rush Medical College and chairperson of the Department of Internal Medicine, is a co-author of the study.
“Turning one's own immune system against cancer using something as available and simple as a flu shot,” he said, “may help certain patients with cancer in the near future, instead of within a decade.”
 Rush University is set to celebrate over 800 graduates at its 53rd commencement ceremony on Saturday, May 3, at Credit Union One Arena.The…
Rush University is set to celebrate over 800 graduates at its 53rd commencement ceremony on Saturday, May 3, at Credit Union One Arena.The… Programs in College of Nursing and College of Health Sciences reinforce commitment to academic excellence through 2024-25 U.S. News & World…
Programs in College of Nursing and College of Health Sciences reinforce commitment to academic excellence through 2024-25 U.S. News & World… Julie Hoff, PhD, RN, FNAP, FAAN, has been selected to serve as the next provost for Rush University. Her selection follows a nationwide search led…
Julie Hoff, PhD, RN, FNAP, FAAN, has been selected to serve as the next provost for Rush University. Her selection follows a nationwide search led… Every year, Rush Medical College’s graduating students gather in March to find out where their careers in medicine will take them next. Just as…
Every year, Rush Medical College’s graduating students gather in March to find out where their careers in medicine will take them next. Just as… For Margaret Bavis, DNP, APRN, FNP-BC, Rush University System for Health is a place that has shaped her family, career and life, beginning long…
For Margaret Bavis, DNP, APRN, FNP-BC, Rush University System for Health is a place that has shaped her family, career and life, beginning long… Andrew Klein, MS, RRT, adult clinical education coordinator and assistant professor, College of Health Sciences, was recently named the 2024…
Andrew Klein, MS, RRT, adult clinical education coordinator and assistant professor, College of Health Sciences, was recently named the 2024…